

Fractures of the second and fourth metacarpal and metatarsal bones (splint bones) are frequently seen in equine practice (Jones and Fessler, 1977; Bowman et al, 1982; Allen and White, 1987). Splint bones are vestigial structures that articulate with the distal carpus and tarsus at their proximal extent, and are tightly adhered to the third metacarpal/ metatarsal bone along their axial margin for the proximal two thirds of the bone. They have a role in stabilising and supporting the carpometacarpal and tarsometatarsal joints via numerous soft tissue attachments, including distal parts of the collateral ligaments of the carpus and tarsus, and in transferring weight from the carpus and tarsus to the third metacarpal and metatarsal bones (cannon bones) respectively, via the interosseous ligament (Peterson et al, 1987; Richardson, 1990; Doran, 1994; Kidd, 2003; Sherlock and Archer, 2008; Lescun, 2021). The most substantial articulation is that of the second metacarpal bone at the carpus, while the fourth metatarsal has the smallest articulation with the tarsus with minimal weight-bearing function (Baxter et al, 1992; Lescun, 2021).
Owing to the splint bones' close approximation with the suspensory ligament (interosseous medius) along their entire length, concurrent injury to both structures is common (Sherlock and Archer, 2008; Nixon and Fortier, 2020). Fractures can occur anywhere along the length of the splint bones, in horses of all ages (Doran, 1994; Jenson et al, 2004; Jackson et al, 2007). Fractures of the splint bones can result from external trauma such as kicks, interference while working, other traumatic injuries, or internal forces associated with desmopathy of the suspensory ligament or excessive traction by fascial attachments during hyperextension of the fetlock joint (Jones and Fessler, 1977; Verschooten et al, 1984; Richardson, 1990; Nixon and Fortier, 2020). The sparse soft tissue covering over the splint bones, as well as their anatomical location, makes them particularly susceptible to external trauma (Harrison et al, 1991; Baxter et al, 1992; Du Preez, 1994; Jackson et al, 2007; Sherlock and Archer, 2008).
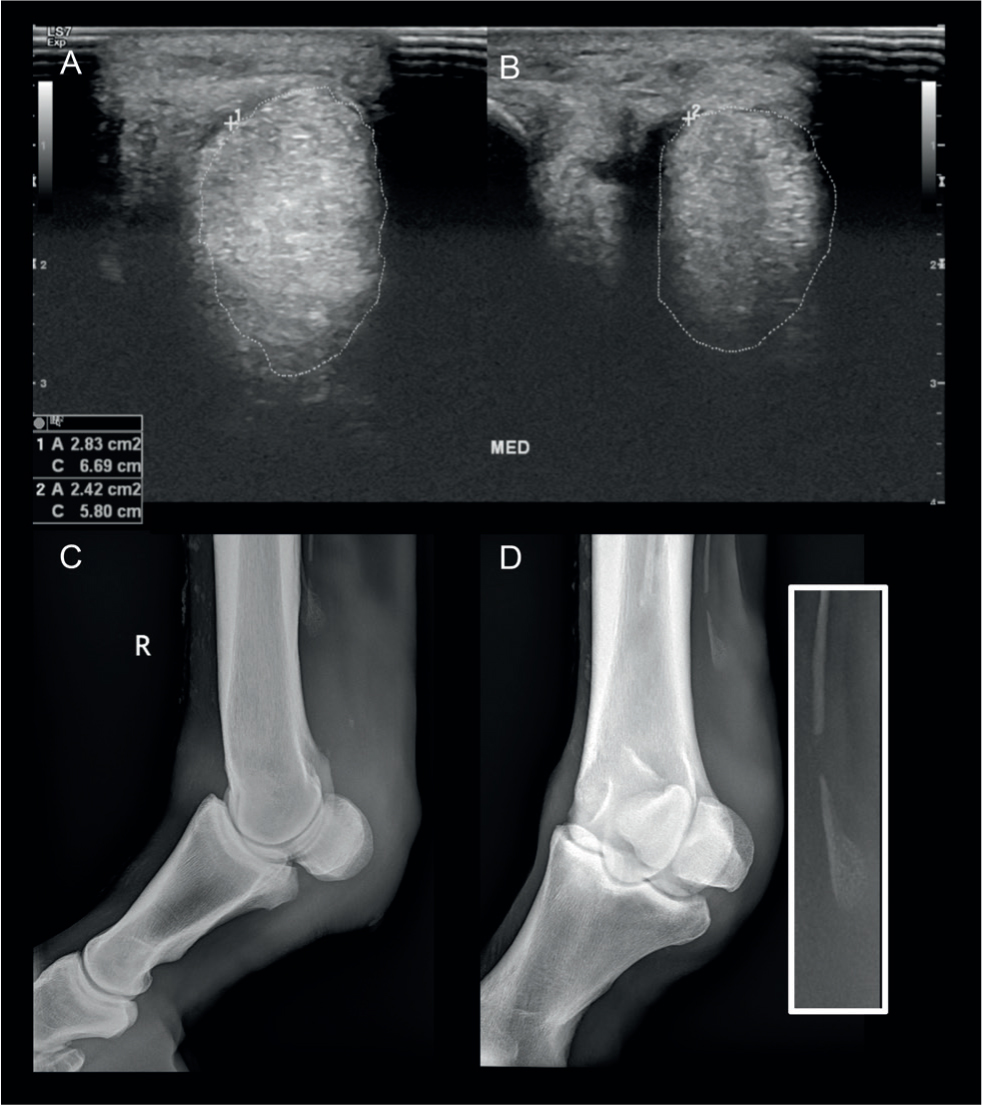
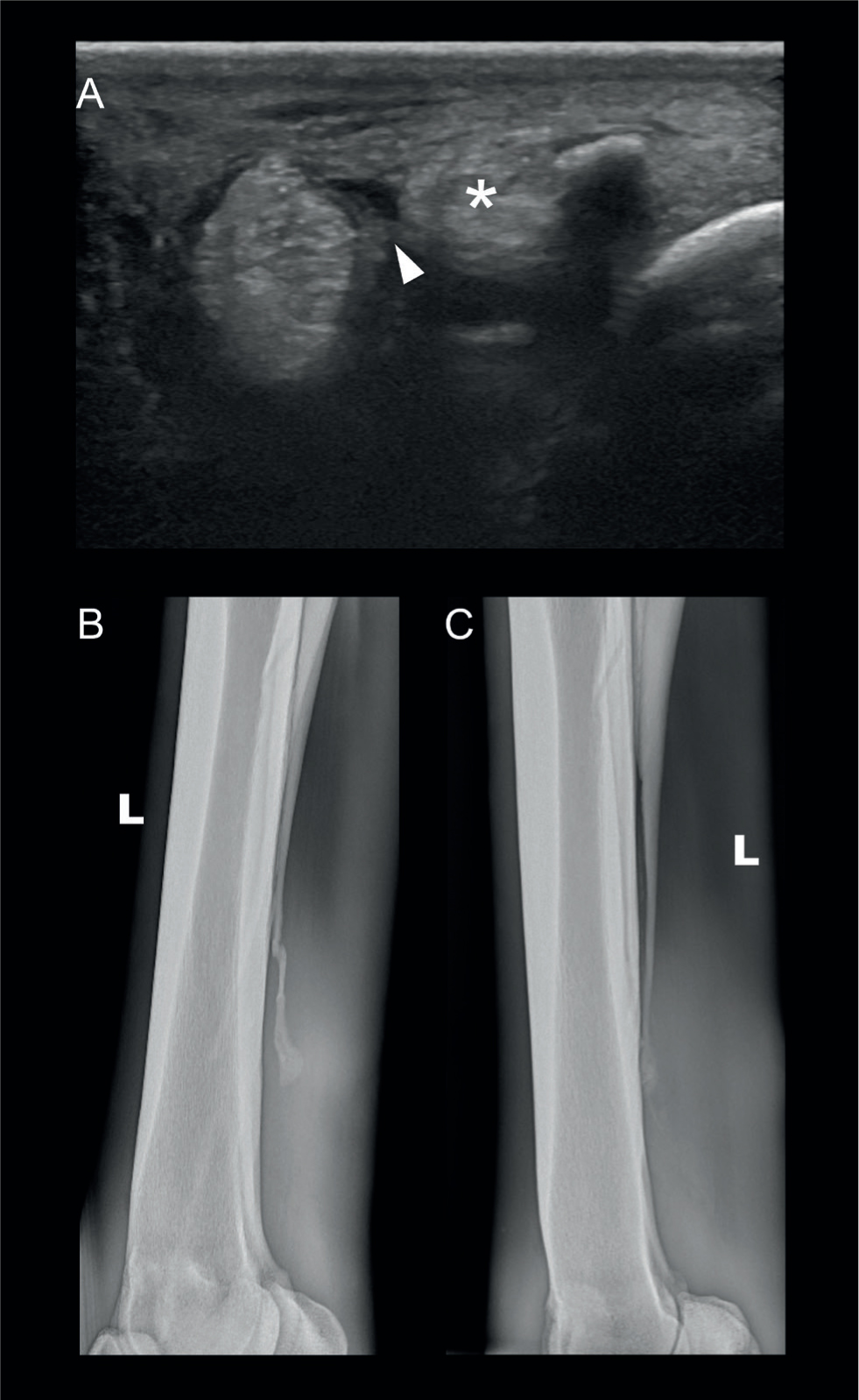
Splint bone fractures are generally characterised by their position and nature, being either proximally, mid-body or distally located, and either simple or comminuted, or open or closed (Richardson, 1990; Jackson et al, 2007; Nixon and Fortier, 2020). The clinical details of the cases discussed in this article are given in Appendix 1. Simple fractures of the distal third of the splint bone are the most common and are frequently associated with internal strain (Jones and Fessler, 1977; Bowman et al, 1982; Verschooten et al, 1984; Doran et al, 1991; Kidd, 2003) (Figure 1). Proximal and middle third fractures are less common and are generally associated with external trauma (Bowman and Fackelman, 1982; Allen and White, 1987; Richardson, 1990; Doran et al, 1991; Harrison et al, 1991; Baxter et al, 1992; Jackson et al, 2007). Horses presenting with acute splint bone fractures often have skin wounds with concurrent desmitis or laceration of the suspensory ligament or injury to the vasculature in the vicinity. Less commonly, they may be associated with cortical fracture of the cannon bone and/or septic arthritis of the tarsometatarsal or distal carpal joints. Concurrent lesions in horses presenting with chronic splint bone fracture include bone sequestrum, osteomyelitis, osteitis, septic arthritis, excessive callus formation and suspensory desmopathy (Bowman and Fackelman, 1982; Allen and White, 1987; Harrison et al, 1991) (Figures 2 and 3).
Although there can be considerable overlap, management strategies for splint bone fractures, categorised as surgical or conservative, are implemented depending on the characteristics of the specific splint bone fracture.
The fundamental principles of treatment are to address the horse's pain, eliminate infection and promote healing. Minimising impingement on the suspensory ligament by callus or fractured bone should be a priority, and can be achieved by either partial splint bone amputation or stabilisation of the fracture, surgically or conservatively. Prognosis is generally good, although concurrent suspensory involvement increases the convalescence period and can be a limiting factor in the outcome of these cases, leading to chronic lameness (Bowman et al, 1982; Richardson, 1990; Doran, 1994; Jackson et al, 2007; Nixon and Fortier, 2020; Lescun, 2021). Horses with traumatic injury to a splint bone should be carefully assessed for concurrent cannon bone fracture before undergoing general anaesthesia as, in these cases, recovery from anaesthesia poses a risk of catastrophic fracture (Jackson et al, 2007; Sherlock and Archer, 2008; Lescun, 2021).
Diagnosis
Clinical examination
Static orthopaedic examination is usually sufficient to identify injury to or raise suspicion of splint bone fracture, but chronic fractures of the splint bone can be relatively quiescent (Bowman et al, 1982). Careful palpation of the splint bones and surrounding tissues usually reveals swelling and/or elicits pain (Kidd, 2003). Wounds overlying splint bones, particularly proximally, should prompt evaluation of the splint bone and adjacent synovial structures (Richardson, 1990). Dynamic orthopaedic evaluation usually reveals lameness in the affected limb, but the degree of lameness depends on the interval between the incident and examination, as well as the extent of soft tissue damage and presence of sepsis (Peterson et al, 1987; Harrison et al, 1991; Jackson et al, 2007). Horses with chronic splint bone fractures and distal splint bone fractures are typically mildly lame or only show transitory lameness (Kidd, 2003). Regional anaesthesia may occasionally be necessary to identify the splint bone fracture as the cause of lameness, typically in chronic cases. Following anaesthesia of the limb distal to the splint bone fracture, a high four-point nerve block or local anaesthetic infiltration just above the callus should desensitise the area (Kidd, 2003; Nixon and Fortier, 2020).
Diagnostic imaging
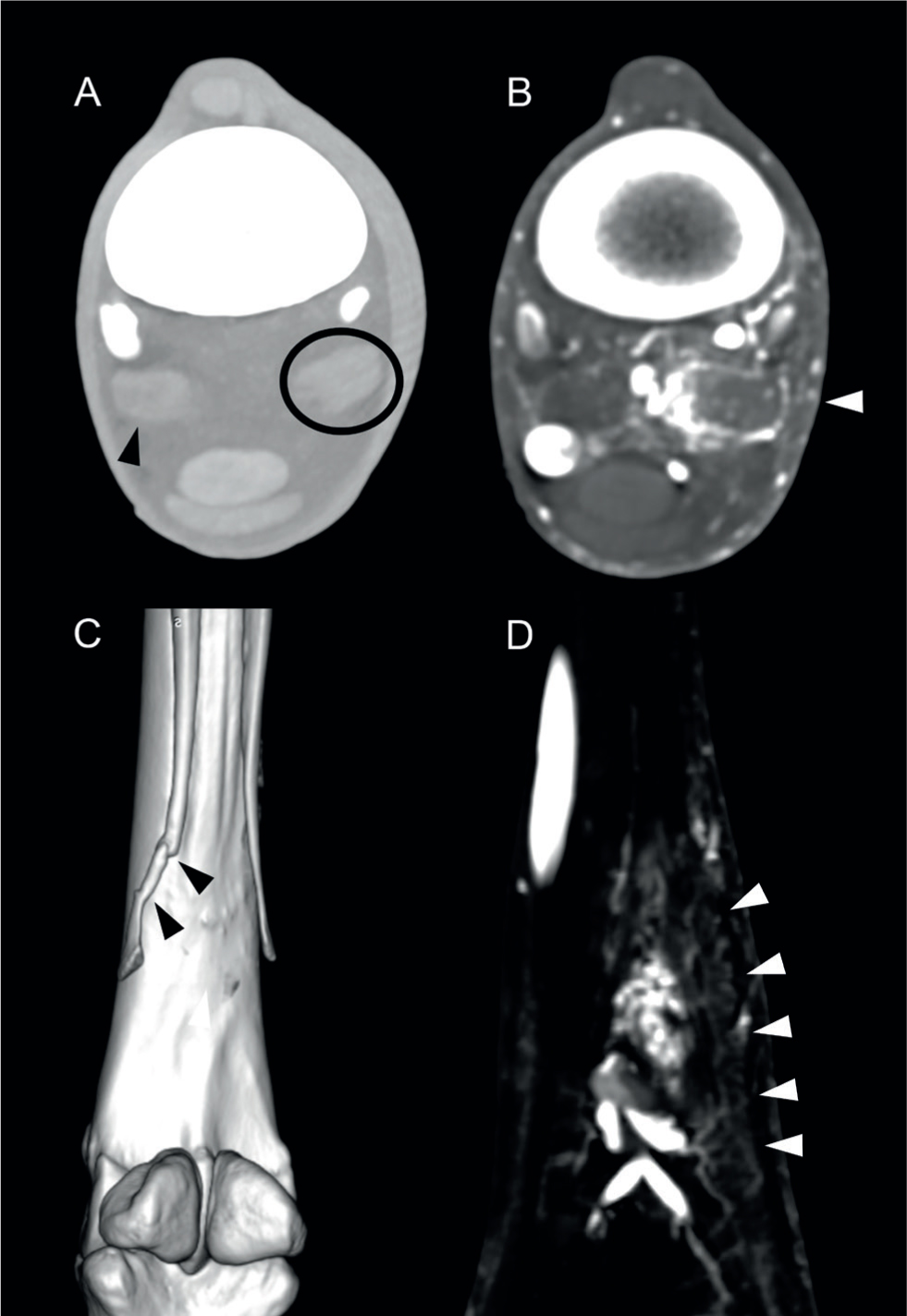
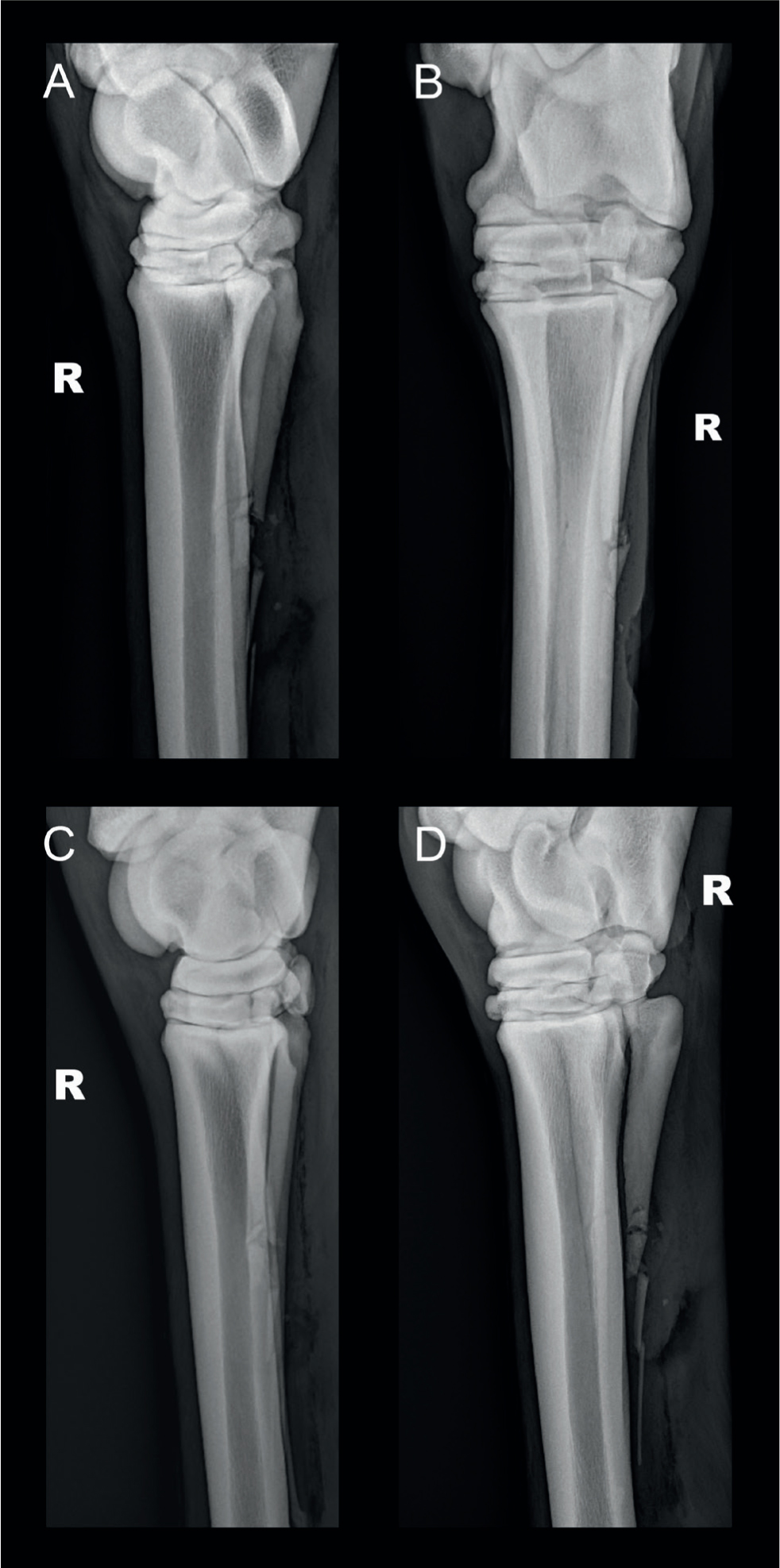
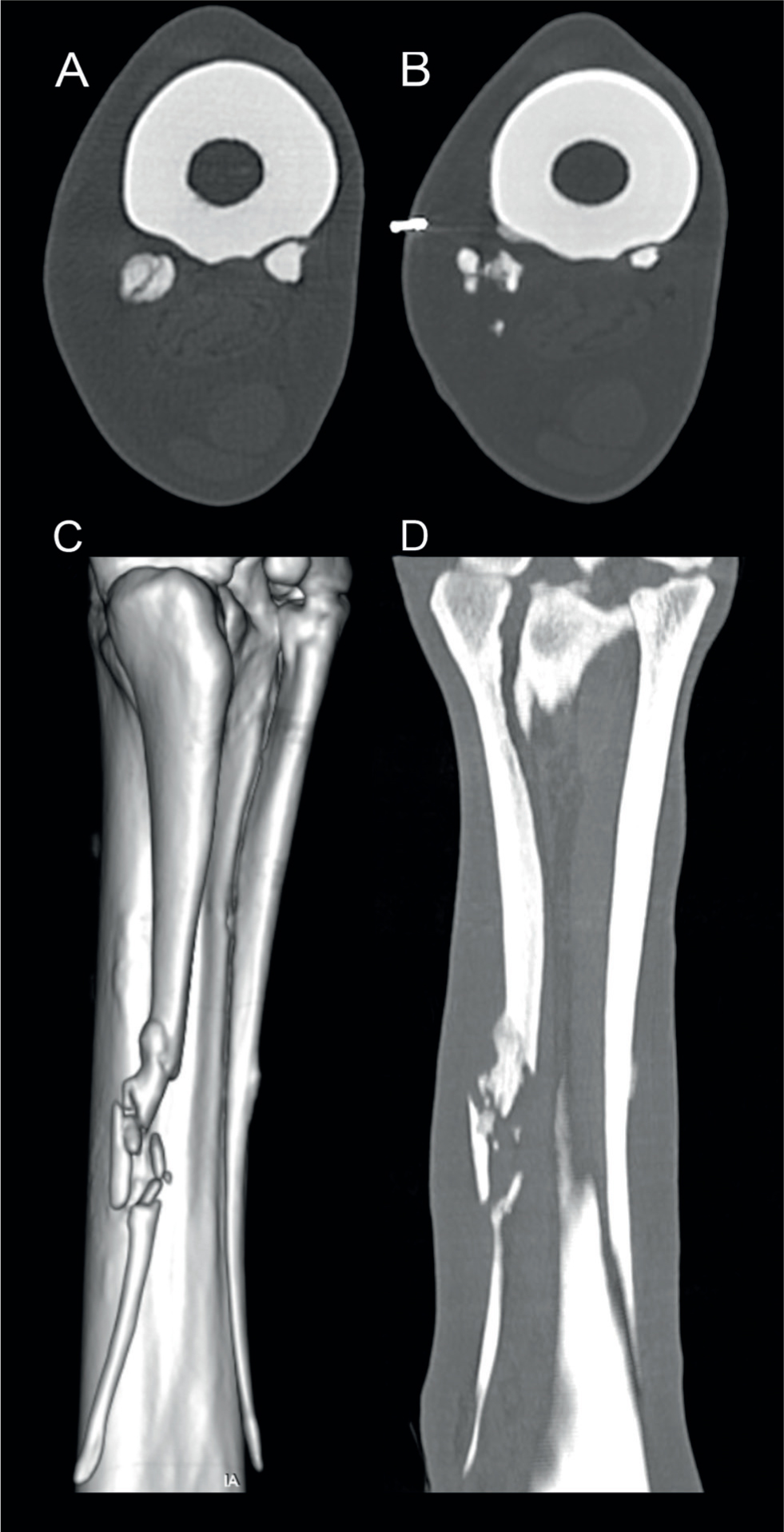
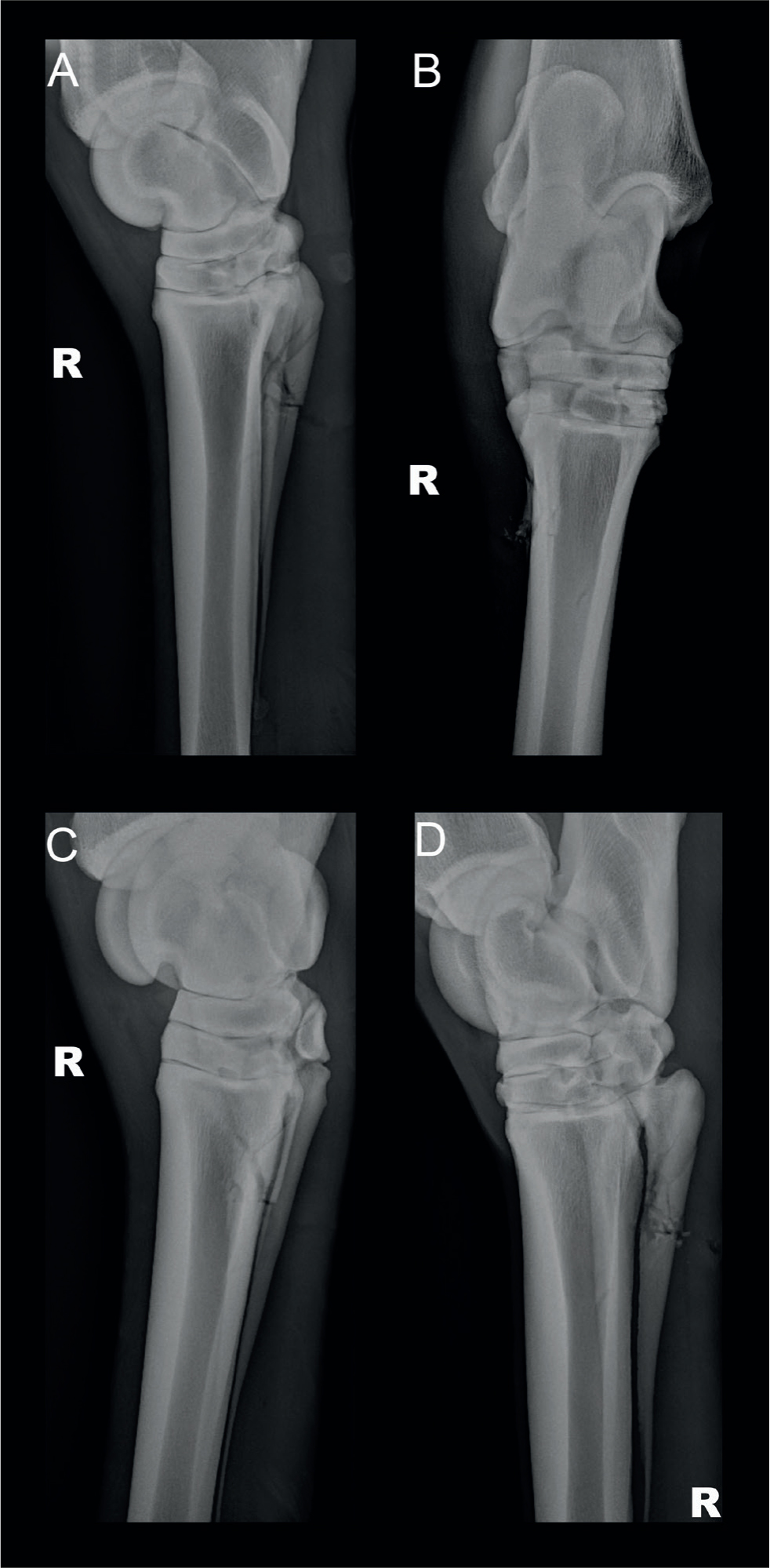
Four radiographic views (dorsopalmar/plantar, lateral and dorsomedial-palmaro/plantarolateral and dorsolateral-palmaro/plantaromedial oblique views) of the metacarpus or metatarsus are usually sufficient to diagnose and characterise most splint bone fractures (Figure 4). Ultrasound examination should be considered as an important additional imaging modality if assessment of the suspensory ligament and other neighbouring soft tissues is indicated (Richardson, 1990; Harrison et al, 1991; Du Preez, 1994; Nixon and Fortier, 2020) (Figure 2). Radiographs should include the carpal and tarsal joints to establish if the fracture is articular (Nixon and Fortier, 2020). It is important to radiographically assess the cannon bone for any concurrent damage, as there are reports of horses suffering catastrophic, complete cannon bone fractures following surgery for splint bone fractures (Jackson et al, 2007; Sherlock and Archer, 2008). In cases in which a concurrent cannon bone fracture is only identified during surgery, the horse should undergo internal fixation, and be recovered with a full limb cast and assisted recovery techniques, depending on the characteristics of the fracture (Lescun, 2021). Advanced imaging such as computed tomography (CT) may be necessary to elucidate some comminuted fractures, identify fissures in the cannon bone and assess adjacent soft tissues (Nixon and Fortier, 2020) (Figures 3 and 5). In a case report by Smith et al (2021), CT identified acute osteomyelitis affecting a traumatised splint bone and a unicortical cannon bone fracture that were not radiographically apparent.
Bacterial sampling
In horses with wounds or evidence of infection, a sample for bacterial culture and sensitivity should be obtained to guide antimicrobial therapy (Kidd, 2003). The most common bacterial isolates from wounds in horses with splint bone fractures include Escherichia coli and Streptococcus spp. These wounds will remain positive for bacterial culture as long as necrotic tissue or bone sequestration remain (Bowman and Fackelman, 1982; Allen and White, 1987; Peterson et al, 1987; Doran et al, 1991; Kidd, 2003).
Conservative management
Conservative management strategies are best suited to minimally displaced splint bone fractures, whether open or closed, simple or comminuted. Treatment consisting of thorough debridement and lavage, with wound closure once contamination has been eliminated, is recommended in horses with open fractures (Richardson, 1990; Archer, 2011; Nixon and Fortier, 2020). Loose bone fragments should be removed at the same time, but it is not appropriate to remove minimally displaced fragments that retain soft tissue attachments. This is usually undertaken in standing sedated horses following administration of appropriate local anaesthesia (Nixon and Fortier, 2020). Analgesia and support bandages are indicated, with stable rest for 6–8 weeks followed by a controlled exercise programme for another 6–8 weeks (Bowman and Fackelman, 1982; Harrison et al, 1991; Jackson et al, 2007; Sherlock and Archer, 2008). Appropriate antimicrobial therapy should be implemented in horses with open fractures, based on the sensitivity patterns of bacterial cultures and the severity of the disease process (Bowen and Slater, 2021).
Horses with associated suspensory desmopathy should be box-rested for 2–3 months, then follow a controlled exercise programme for 6–8 months depending on the severity of the lesion and the progression of healing (Verschooten et al, 1984). Regular ultrasound examination should be undertaken to assess healing. It is recommended to re-radiograph box-rested horses at 4–6-week intervals, or with any change in the degree of lameness, as displacement can occur as a late event and may require surgical management (Richardson, 1990). One study of 53 horses reported that conservative management of open comminuted fractures of the proximal third of the fourth lateral splint bone had comparable convalescent periods, survival rates and return to full work as those in surgically managed patients (Sherlock and Archer, 2008).
Surgical management
Surgical treatment is indicated for the removal of sequestered bone or bone fragments, lavage of infected synovial structures, debridement of areas affected with osteomyelitis, and for aggressive wound management (Bowman and Fackelman, 1982; Allen and White, 1987; Peterson et al, 1987; Richardson, 1990; Harrison et al, 1991; Baxter et al, 1992; Doran, 1994; Du Preez, 1994; Kidd, 2003; Jenson et al, 2004; Milner, 2008; Mageed et al, 2018; Nixon and Fortier, 2020). Surgical management may also be selected to minimise callus formation, either by improving the stability of the fracture with internal fixation, or by amputation of part of the splint bone. Fractures affecting the proximal portion of the splints can be repaired with internal fixation (Peterson et al, 1987; Richardson, 1990; Sherlock and Archer, 2008; Mageed et al, 2018; Nixon and Fortier, 2020). One study found that horses with acute splint bone fractures presenting without associated suspensory desmopathy that underwent early surgical management avoided the occurrence of suspensory desmopathy (Bowman and Fackelman, 1982). A commonly used surgical technique is to remove the distal portion of the splint bone including the fracture plane (Bowman and Fackelman, 1982; Allen and White, 1987; Richardson, 1990; Du Preez, 1994; Kidd, 2003; Jackson et al, 2007; Milner, 2008; Sher-lock and Archer, 2008; Nixon and Fortier, 2020) (Figure 6).
Following surgery, horses without concurrent suspensory desmopathy should be box-rested until suture removal and hand walked for a further 30 days (Kidd, 2003). After 30 days, horses can be turned out into a small paddock (Bowman et al, 1982). In uncomplicated cases, controlled exercise can be reinstated 2 months postoperatively and horses can return to full work 4 months postoperatively (Allen and White, 1987). Horses with suspensory desmopathy require 3–9 months of rest with regular ultrasound examinations to monitor healing of the suspensory ligament (Kidd, 2003). Cosmetic results post-surgery are reported as excellent (Allen and White, 1987; Sherlock and Archer, 2008; Nixon and Fortier, 2020).
Distal third splint bone fractures
Distal splint bone fractures are the most common splint bone fracture. Fractures occur with greater frequency in forelimbs compared to hindlimbs and can be caused by either internal or external forces (Bowman et al, 1982; Verschooten et al, 1984; Jack-son et al, 2007; Nixon and Fortier, 2020). The distal aspect of the splint bone is superficially located and is therefore vulnerable to external trauma (Nixon and Fortier, 2020) (Figures 2 and 3). Internal trauma induced by fetlock flexion and extension can strain and ultimately fracture the distal splint, and is exacerbated by suspensory branch enlargement (Figure 1). An experimental study demonstrated that hyperextension of the fetlock joint resulted in increased tension on the interosseus ligaments and a band of soft tissue that extends from the distal aspect of the splint bones to the proximal sesamoid bones, resulting in fracture of the distal part of the splint bone (Verschooten et al, 1984). Abaxial strain is placed on the distal splint bones during fetlock flexion and can be exaggerated by enlargement of the suspensory ligament (Verschooten et al, 1984; Nixon and Fortier, 2020). The findings of two studies highlight the relationship between suspensory desmopathy and distal splint bone fracture. Most horses in these studies presenting for distal splint bone fracture had concurrent suspensory desmopathy (Bowman et al, 1982; Verschooten et al, 1984).
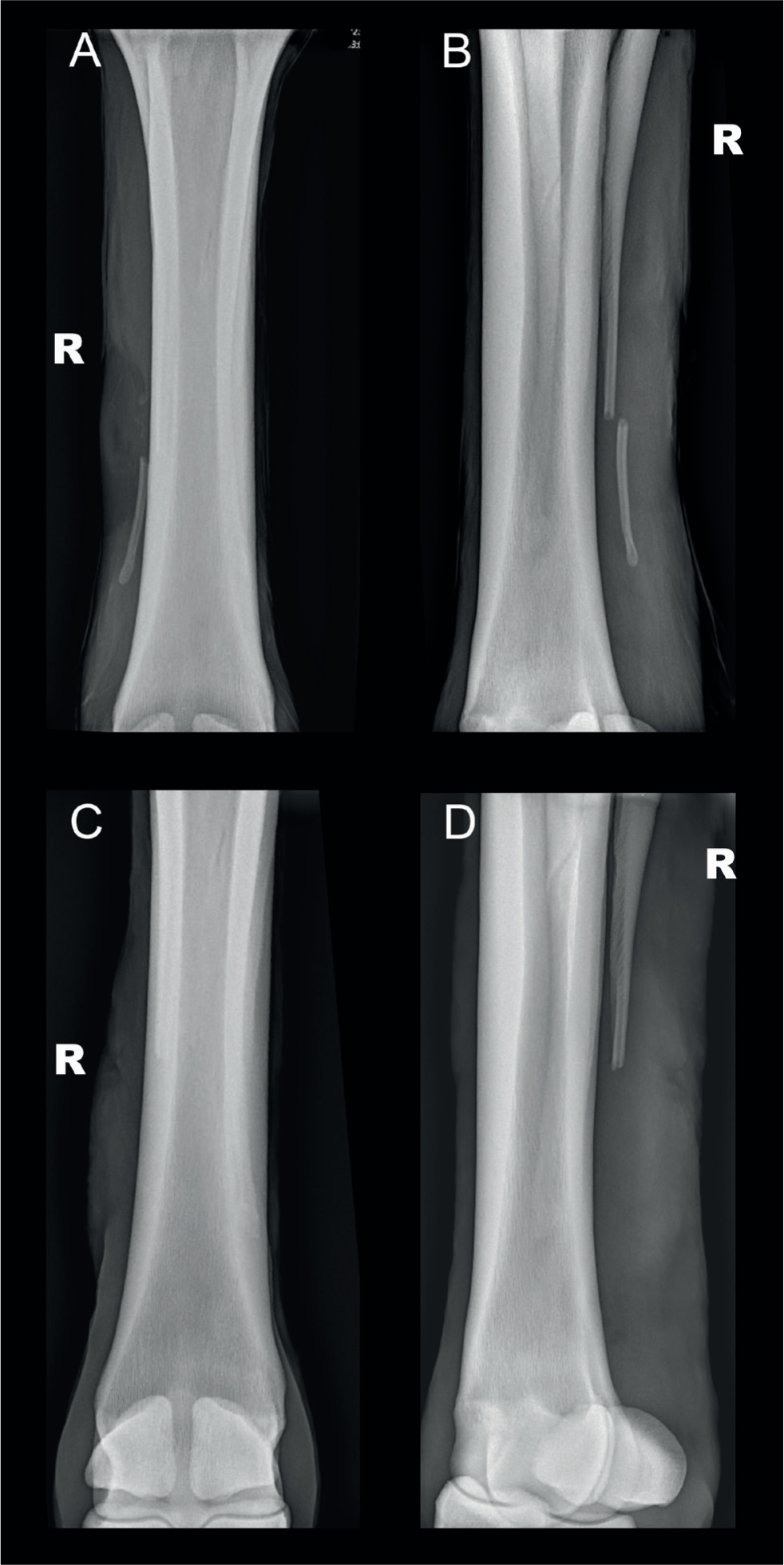
Distal splint bone fractures are rarely open or comminuted. Acute fractures often appear as simple, complete, slight oblique fractures radiographically (Jackson et al, 2007; Nixon and Fortier, 2020) (Figure 6). In more chronic cases, a callus can form and impinge on the adjacent suspensory ligament (Nixon and Fortier, 2020) (Figure 3).
Treatment for distal splint bone fractures consists broadly of either surgical excision of the distal splint or conservative management – rest and bandaging. Many simple fractures develop a functional fibrous or osseous union with only transient lameness (Nixon and Fortier, 2020). A minimum of 2 months' box rest results in sufficient healing for most distal fractures. Complete union can occur within 2 months, but thickening of the healed, distal portion of the splint bone is a consistent feature (Verschooten et al, 1984). Potential complications of conservative management include exuberant callus formation, which could interfere with the suspensory ligament, non-union (possibly owing to the continuous or intermittent tension on the distal aspect of the splint bones by the soft tissue attachments), or refracture (Bowman and Fackelman, 1982; Verschooten et al, 1984; Baxter et al, 1992; Lescun, 2021). A retrospective study found that conservative therapy was more cost effective compared to surgical treatment, but required a longer convalescence period and was subject to more complications, particularly exuberant callus formation (Jackson et al, 2007).
The risk of exuberant callus formation and prolonged convalescence is reduced by early removal of the distal fractured portion (Nixon and Fortier, 2020). Open and displaced fractures generally require surgical management (Doran, 1994). The surgical procedure is simple and can often be performed in the standing sedated horse (Stack et al, 2016; Nixon and Fortier, 2020). Surgical management comprises the removal of the distal fragment of the fractured splint bone, removal of the callus and tapering of the most distal portion of the remaining proximal fragment (Allen and White, 1987; Doran, 1994; Jackson et al, 2007) (Figure 6). Complications after distal splint bone amputations are rare, but can include the development of periosteal proliferative changes at the distal aspect and surgical site infection (Jackson et al, 2007).
Middle third splint bone fractures
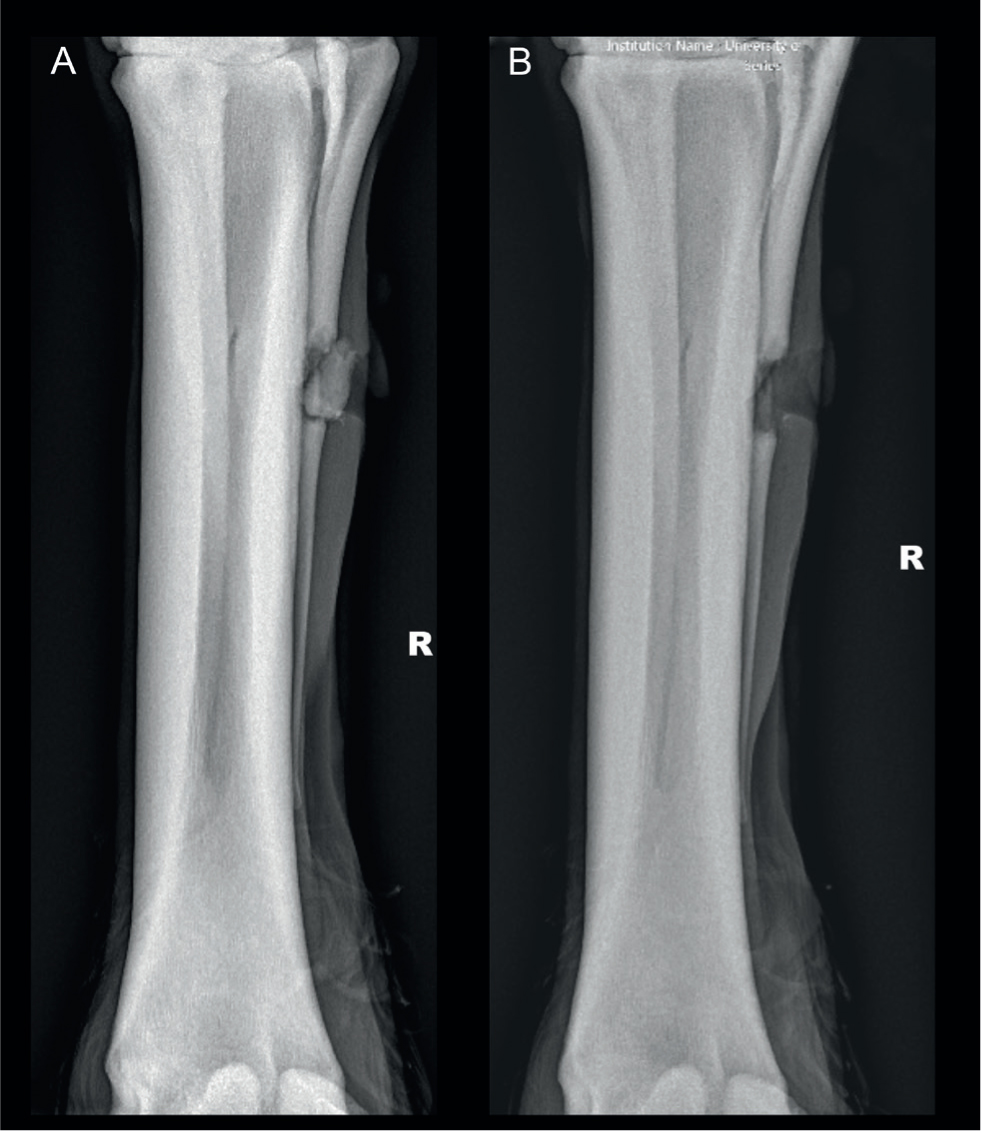
Fractures to the mid-body and proximal thirds are less common than distal splint bone fractures and are mostly caused by known external trauma such as kicks or interference while working, or as sequelae to osteomyelitis from penetrating wounds (Allen and White, 1987; Peterson et al, 1987). Mid-body fractures are often open and frequently have a complex configuration (Baxter et al, 1992) (Figure 4 and 5). The suspensory ligament is less likely to be involved than with distal splint bone fractures, although exuberant callus formation seen in chronic fractures can adhere to or impinge the suspensory ligament (Nixon and Fortier, 2020). Conservative management consisting of stable rest, anti-inflammatory or analgesic therapies, and supportive bandaging or casting may be successful, but exuberant callus formation impinging on the suspensory ligament can result in lameness (Nixon and Fortier, 2020).
Conservative management of mid-body fractures should be considered in non-displaced fractures, or if healing is already progressing at the time of diagnosis. Open infected fractures can be successfully treated with antimicrobials, but if the infection returns after cessation of the antimicrobials, further radiography is indicated to identify potential sequestra or osteomyelitis (Jackson et al, 2007). Sequestrated and infected bone should be removed surgically. It has been suggested that open and/or displaced fractures should be treated with surgical management (Jenson et al, 2004).
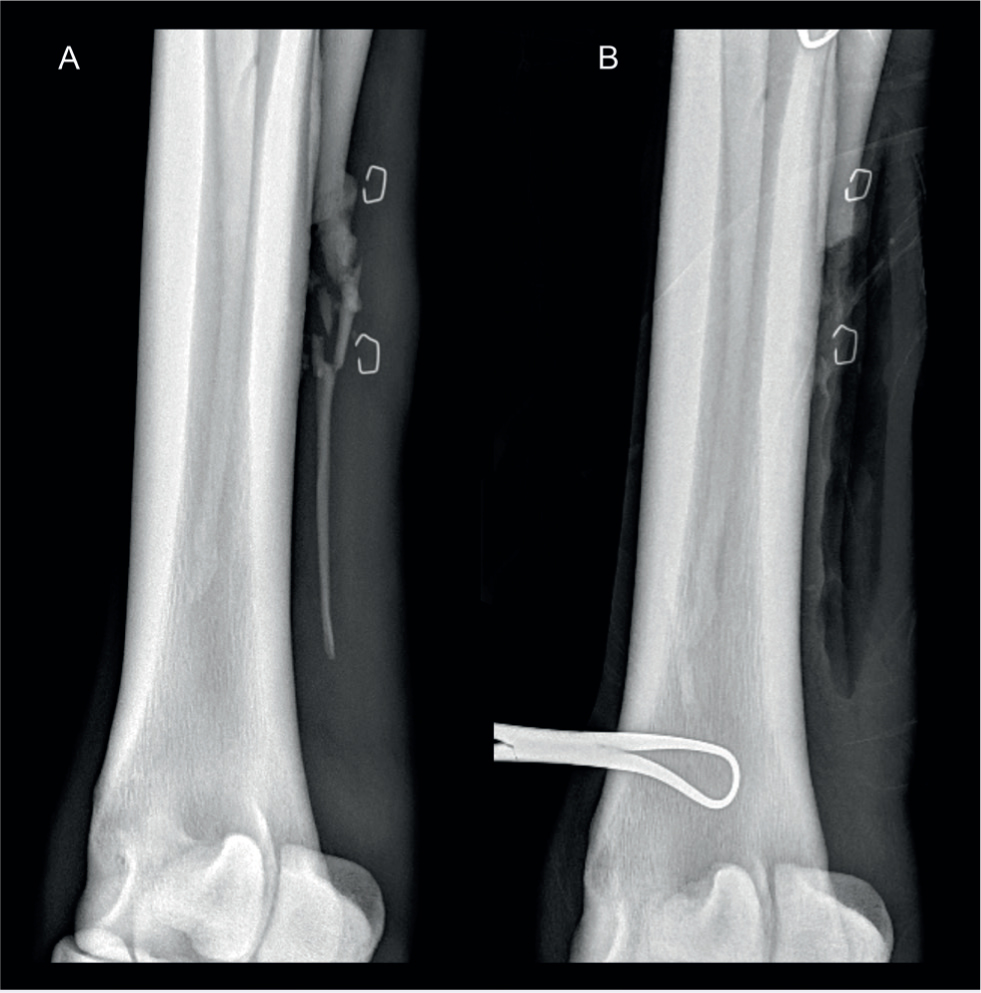
Surgical management of mid-body fractures mirrors that of distal splint bone treatment and comprises oblique ostectomy just proximal to the fracture callus, which allows removal of the fractured distal portion of the splint as well as the fracture and callus (Bowman et al, 1982; Nixon and Fortier, 2020) (Figure 7). It is generally accepted that up to two thirds of the splint bone can be removed without compromising axial support (Peterson et al, 1987; Richardson, 1990; Jackson et al, 2007; Mageed et al, 2018). Segmental ostectomy, where only the affected portion of the splint bone and any surrounding affected soft tissue or callus is removed and the proximal and distal splint bones remain in place, has also been described, with successful return to previous performance levels (Jenson et al. 2004) (Figure 8).
Proximal third splint bone fractures
Fractures of the proximal third of the splint bones are usually the result of trauma and consequently, fractures are typically open and comminuted, with the fourth metacarpal and metatarsal overrepresented in these cases (Bowman and Fackelman, 1982; Doran, 1994; Jackson et al, 2007; Nixon and Fortier, 2020) (Figure 9). Closed fractures can occur and usually present with heat, swelling and lameness. Open fractures present with severe lameness, wounds or draining tracts (Allen and White, 1987). Open proximal splint bone fractures can result in synovial sepsis of the carpometacarpal or tarsometatarsal joint with bacteria gaining access to the joint either directly via the wound or indirectly via the fracture plane (Baxter et al, 1992).
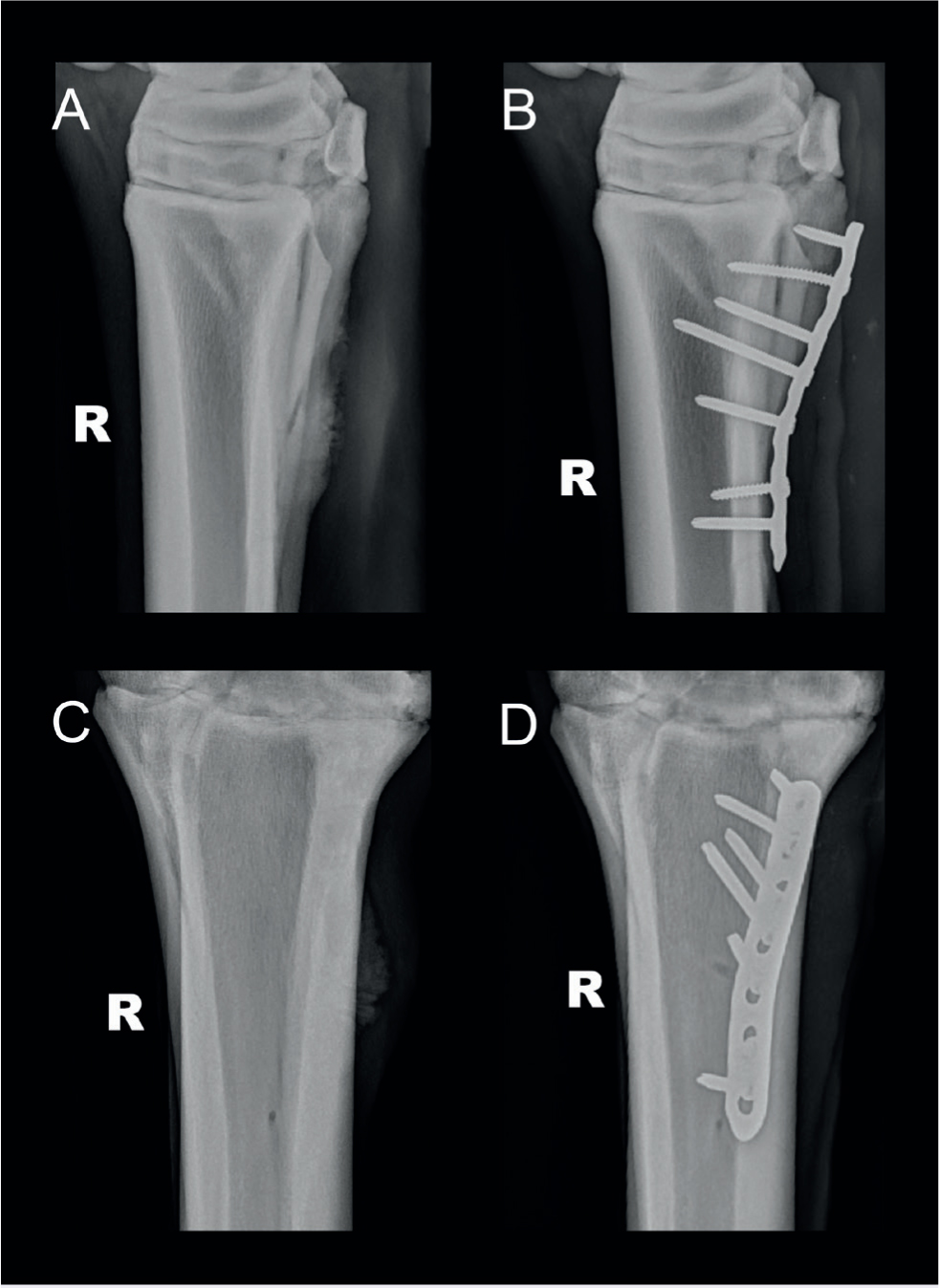
Conservative management of proximal splint bone fractures consisting of analgesia, anti-inflammatories, supportive bandages or casts and local wound therapy is possible, but can be unrewarding, leading to non-unions, excessive callus formation, sequestrum formation and/or chronic lameness (Bowman and Fackelman, 1982; Allen and White, 1987; Peterson et al, 1987). However, conservative management of proximal comminuted open fourth metatarsal fractures can be as successful as surgical management and is not as financially onerous. A multicentre case series comparing 21 horses treated conservatively and 32 treated surgically with open comminuted proximal fourth metatarsal fractures had comparable outcomes in return to athletic function and duration of convalescence (Sherlock and Archer, 2008). Internal stabilisation of fourth metatarsal proximal fractures is not always necessary as the fourth metatarsal only has a small proximal articulation and is subject to a lower axial load than other splint bones (Sherlock and Archer, 2008). In contrast, the medial splint bones articulate fully with the second carpal or tarsal bone and are subject to greater axial load. Subsequently, stabilisation of proximal fractures of medial splint bones is advised (Figure 10).
Surgical options for proximal splint bones include segmental ostectomy, sequestrectomy, removal of the fracture fragments and distal part of the bone, internal fixation of the fracture or complete extirpation of the fourth metatarsal (Bowman and Fackelman, 1982; Allen and White, 1987; Sherlock and Archer, 2008). One study reported that complete removal of the fourth metatarsal was used to treat open comminuted fractures of the proximal aspect of the fourth metatarsal, with 5 out of 8 horses returning to their intended use (Baxter et al, 1992). Complete removal of the medial splint bone is not recommended because of the the risk of subluxation or luxation of the distal carpal or tarsal joints (Baxter et al, 1992; Nixon and Fortier, 2020).
Strategies for surgical repair depend on the fracture characteristics. Displaced proximal splint bone fractures, whether open or closed, particularly if the fractures are articular, should ideally be treated with open reduction and internal fixation, ensuring all infected or necrotic tissue is removed (Richardson, 1990). Some authors report that surgical removal of the distal fragment and associated callus should be undertaken for proximal fractures (Bowman and Fackelman, 1982; Allen and White, 1987). However, sequelae to the removal of more than two thirds of the splint bone include displacement or comminution of the proximal fragment and excessive motion of the remaining segment during weight-bearing. These can lead to suspensory desmitis and degenerative joint disease of the carpometacarpal and tarsometatarsal joints respectively (Bowman and Fackelman, 1982; Peterson et al, 1987).
In cases where more than two thirds of the splint bone has to be removed, internal fixation of the proximal fragment to the cannon bone has been suggested to help maintain axial support (Bowman and Fackelman, 1982). The need for internal fixation should be determined during surgery using digital palpation. If the interosseous attachments between the proximal segment and the cannon bone are unstable, internal fixation should be used (Peterson et al. 1987). Internal stabilisation of the remaining proximal portion of the splint bone can be achieved with screw fixation to the cannon bone (Bowman and Fackelman, 1982; Allen and White, 1987), or plate fixation (Peterson et al, 1987; Nixon and Fortier, 2020) (Figure 10).
A study comparing screw fixation to plate fixation of the proximal third of the splint bone found that screw fixation alone had a high prevalence of technical failure and a guarded prognosis for soundness; with only 2 out of 11 horses studied becoming sound for their intended use (Peterson et al, 1987). Comparatively, favourable results were obtained with plate fixation and 6 out of 11 horses that underwent plate fixation became sound for their intended use, with a low incidence of technical failure (Peterson et al, 1987). Some splint bone fracture configurations are amenable to plate stabilisation where the screws do not engage the cortex of the cannon bone (Peterson et al, 1987; Nixon and Fortier, 2020). Internal fixation can be undertaken in open fractures despite an increased risk of infection, or even in the face of an already established infection (Allen and White, 1987; Peterson et al, 1987; Richardson, 1990; Harrison et al, 1991; Du Preez, 1994; Nixon and Fortier, 2020).
Peterson et al (1987) reported that plate fixation maintained fracture alignment in 4 horses from which positive culture results were obtained. Another study suggested that the use of bioabsorbable screws for fixation of the proximal portion of the splint bone after the distal two thirds were resected was a safe and feasible technique and reported favourable results, with no complications encountered postoperatively and 6 out of 8 horses returned to their intended use (Mageed et al, 2018).
Prognosis
The prognosis following splint bone fractures depends on the location, configuration and age of the fracture and additional involvement of adjacent soft tissues, joints and the cannon bone. Fractures of the distal and middle thirds of the splint bone, when no other structures are involved, have the best prognosis (Jackson et al, 2007; Nixon and Fortier, 2020). Concurrent involvement of the suspensory ligament has been implicated as a major limiting factor for return to previous performance (Bowman et al, 1982; Richardson, 1990; Doran, 1994; Kidd, 2003; Jackson et al, 2007; Nixon and Fortier, 2020; Lescun, 2021). Results suggest that return to athletic performance following plate fixation for proximal third splint bone fractures is fair, with 6/11 horses returning to their intended use (Peterson et al, 1987).
Conclusions
Successful outcomes in horses with splint bone fractures can be achieved with both conservative and surgical strategies, but both approaches have advantages and disadvantages. The position of the fracture (proximal, middle or distal) may dictate the therapeutic strategy implemented. Conservative management is less invasive and less expensive than surgery and may be initially attempted in many splint bone fractures, particularly non-displaced fractures, and fractures not requiring extensive debridement or wound reconstruction. The main complication following conservative management is callus formation with impingement on the suspensory ligament, which can result in lameness and may require surgical intervention and prolonged convalescence. Surgical management often requires general anaesthesia and is more costly, but can result in shorter convalescence and fewer long-term complications. Currently, many authors indicate a preference for surgical management, especially for mid-body and proximal splint bone fractures, and in displaced fractures. The exception is the fourth metacarpal bone, which shows comparable outcomes when treated either surgically or conservatively. A prospective study comparing conservative management to surgical management in matched cohorts would be beneficial to provide further clinical guidance.
KEY POINTS
- Splint bone fractures are commonly encountered in equine veterinary practice and occur along the length of the second and fourth metacarpal and metatarsal bones. Suspensory ligament injury may occur at the time of fracture or later from impingement from bony calluses. Conversely, chronic suspensory ligament enlargement may result in fracture of the distal splint bone.
- Four radiographic views of the metacarpus or metatarsus are usually sufficient to characterise the fracture. Horses with traumatic injury to a splint bone should be carefully assessed for concurrent cannon bone fracture before undergoing general anaesthesia, as recovery poses a risk of catastrophic fracture in these horses.
- Ultrasound should also be performed to investigate any involvement of the suspensory ligament, as this could be a limiting factor for return to previous performance. Computed tomography can yield additional information and should be considered in complex cases.
- Conservative management is successful in some cases, but potential complications include non-union, exuberant callus formation, increased convalescent period, chronic lameness or refracture.
- Surgery often comprises removal of the splint bone distal to the fracture for mid-body and distal fractures. Up to two thirds of the splint bone can be removed without compromising axial limb support. Sequelae to the removal of more than two thirds may include displacement or comminution of the proximal fragment leading to suspensory desmitis and degenerative joint disease of the carpometacarpal and tarsometatarsal joints. Internal fixation should be considered in horses with unstable splint bones following removal of two thirds or more.
- The fourth metatarsus is the splint bone most frequently fractured and has comparable outcomes whether treated conservatively or surgically. Unlike the other splint bones, it can be completely extirpated.
- Prognosis is generally good, but concurrent suspensory desmitis increases the convalescence period and can be a limiting factor in the outcome of these cases as it can lead to chronic lameness.
Table 1. Details of the cases that are presented in the figures.
| Figure | Signalment | Time from injury | Limb and location | Type of fracture | Open/closed | Inciting cause | Degree of lameness | Reason for referral | Main therapy: Surgical or conservative | Outcome if known |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 20 years, Irish draught horse, Gelding | > 6 months | Right hind, fourth metatarsal bone, distal | Simple, displaced | Closed | Chronic suspensory disease and fetlock hyperextension | Mild but worse with flexion | Multi-limb lameness | Conservative: rest, support bandaging and non-steroidal anti-inflammatory drugs | Euthanised as a result of comorbidities |
| 2,3 | 3 years, Irish Sport Horse, Mare | 3 months | Left hind limb, second metatarsal, distal | Comminuted, displaced | Open initially, closed at presentation | Metatarsus stuck under gate, resulting in biaxial trauma | Low grade at trot | Ongoing lameness | Conservative: rest, support bandaging and non-steroidal anti-inflammatory drugs | Remained lame as a result of suspensory adhesion to injured (not fractured) medial splint |
| 4 | 10 years, Welsh C, Mare | <1 day | Right hind, fourth metatarsal bone, mid-level | Severely comminuted, and moderately displaced | Open | Kick from another horse with shoes | Lame at walk | Investigation, treatment of wound | Conservative: including removal of loose fragments and suturing of the wound standing | Discharged from hospital |
| 5,7 | 13 years, New Forest, Mare | 2 weeks | Left hind, fourth metatarsal bone, mid-level | Severely comminuted, and moderately displaced | Open initially, closed at presentation | Suspected kick from another horse | Sound at walk, lame at trot | Ongoing lameness | Surgical: excision of fracture fragments just proximal to the fracture | Discharged from hospital |
| 6 | 15 years, Cob, Mare | <1 day | Right hind, fourth metatarsal bone, distal | Simple, displaced | Open | Suspected kick from another horse | Sound at walk, not trotted | Arterial bleed | Surgical: resection of the distal fragment under general anaesthetic | Discharged from hospital |
| 8 | 7 years, Connemara pony, Gelding | <1 day | Right hind, fourth metatarsal bone, mid-level | Comminuted, displaced | Open | Kick from another horse with shoes | Sound at walk, not trotted | Radiography | Surgical: segmental ostectomy | Discharged from hospital |
| 9 | 13 years, Welsh D, Mare | <1 day | Right hind, fourth metatarsal bone, Proximal | Comminuted, minimally displaced, non-articular | Open | Kick from another horse | Lame at walk | Wound, possible synovial sepsis | Conservative: rest, support bandaging, antimicrobials and non-steroidal anti-inflammatory drugs | Discharged from hospital |
| 10 | 12 years, Irish Sport Horse, Gelding | 2 months | Right hind, second metacarpal bone, within the proximal third | Simple, oblique, non-displaced, non-articular | Closed – scar present | Suspected kick from another horse | Sound at walk, lame at trot | Marked callus formation – suspected suspensory impingement | Surgical: amputation of 3/4 of the second metacarpal bone, followed by stabilisation of the remaining splint with 3.5mm locking compression plate, with systemic antimicrobials and non-steroidal anti-inflammatory drugs | Discharged from hospital |